

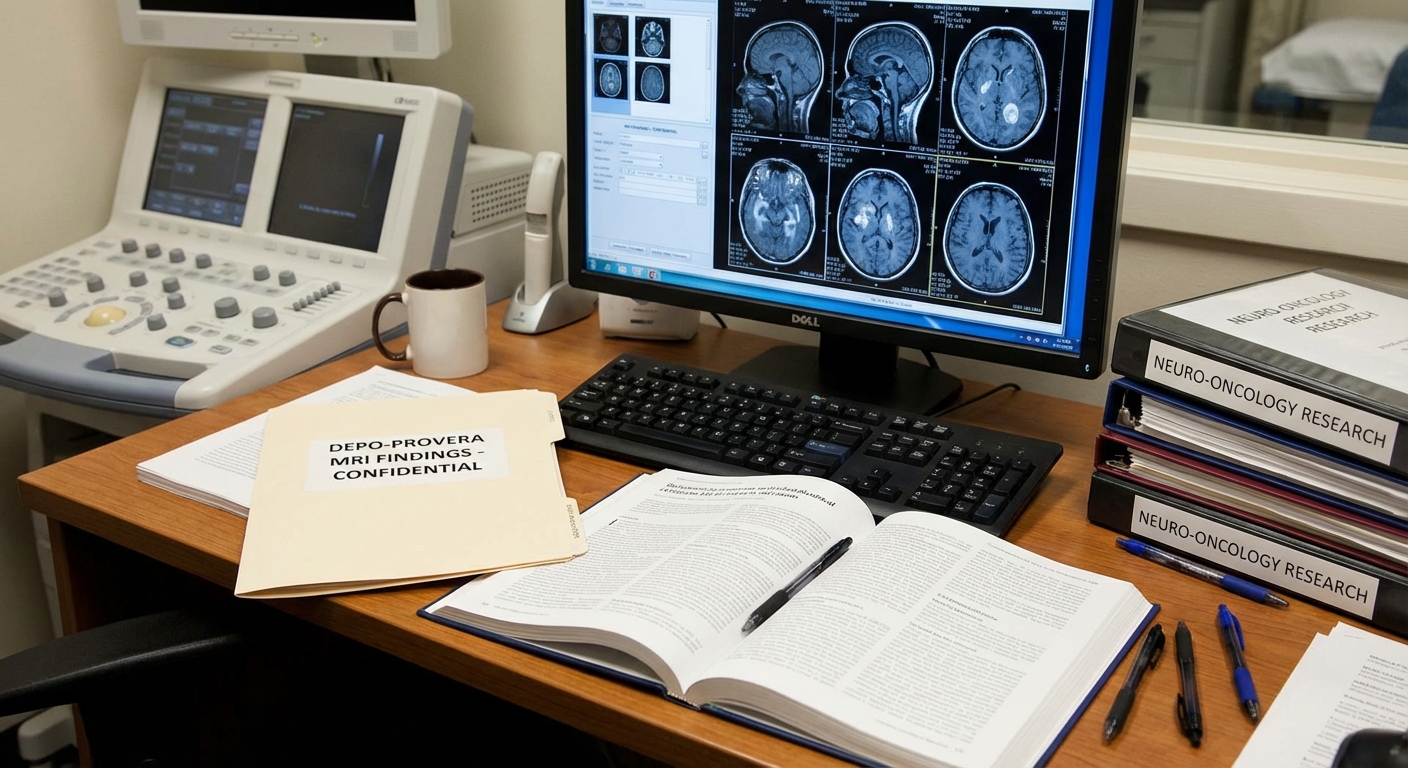
MRI and other imaging play a central role in diagnosing meningiomas. In Depo-Provera litigation, imaging findings are often used to establish timing and location of tumors. Here we explain what is typically at issue.
Magnetic Resonance Imaging (MRI) plays a crucial role in diagnosing meningiomas, the brain tumors that have been linked to long-term Depo-Provera use. Understanding what MRI findings may indicate in Depo-Provera brain tumor cases can help women who have used the medication understand their diagnosis and potential legal rights.
Recent research has revealed a connection between long-term Depo-Provera use and the development of meningiomas, tumors that form on the protective layers surrounding the brain and spinal cord. A landmark French study found that women who used high-dose progestogen medications like Depo-Provera for extended periods faced significantly elevated risks of developing these tumors. MRI scans are typically used to detect and evaluate these tumors, providing important information about their size, location, and characteristics.
Pharmaceutical products and medical research documents
What Are Meningiomas?
Meningiomas are tumors that form on the meninges, the protective layers surrounding the brain and spinal cord. While typically non-cancerous, they can cause serious symptoms as they grow. These tumors develop from cells in the meninges and can vary in size and location, which affects both symptoms and treatment options.
The National Brain Tumor Society notes that meningiomas account for roughly one-third of all primary brain tumors in adults—context that helps readers understand why even a modest relative risk increase can affect many patients.
According to FDA approval history, Depo-Provera (medroxyprogesterone acetate injectable suspension) has been marketed in the United States since 1992, with labeling updated multiple times as progestin safety data evolved.
The National Brain Tumor Society notes that meningiomas account for roughly one-third of all primary brain tumors in adults—context that helps readers understand why even a modest relative risk increase can affect many patients.
Common symptoms of meningiomas include persistent headaches, vision problems, hearing loss or ringing in ears, memory difficulties, seizures, weakness in limbs, and personality changes. The severity of symptoms often depends on the size and location of the tumor. Some meningiomas may cause no symptoms and are discovered incidentally during imaging for other conditions, while others can lead to significant neurological problems requiring immediate treatment.
Don't wait on your Depo-Provera claim—statutes of limitations may apply.
Get a free Depo-Provera case review and learn whether you may qualify.
See if you qualify for a Depo-Provera lawsuitThe National Brain Tumor Society notes that meningiomas account for roughly one-third of all primary brain tumors in adults—context that helps readers understand why even a modest relative risk increase can affect many patients.
According to WHO classification data, meningiomas are typically graded WHO Grade I tumors, yet surgical resection rates climb when tumors enlarge or compress critical structures.
Meningiomas are the most common type of primary brain tumor, accounting for approximately one-third of all brain tumors. While most are benign, they can still cause serious health issues depending on their location and size. Treatment options may include monitoring, surgery, radiation therapy, or a combination of approaches depending on the individual case.
How MRI Detects Meningiomas
MRI scans use powerful magnets and radio waves to create detailed images of the brain and surrounding structures. These scans are particularly effective at detecting meningiomas because they provide clear visualization of the meninges and can show tumors that may not be visible on other types of imaging.
The National Brain Tumor Society notes that meningiomas account for roughly one-third of all primary brain tumors in adults—context that helps readers understand why even a modest relative risk increase can affect many patients.
According to CDC National Health Statistics Reports, injectable contraceptives are used by roughly 2% to 3% of U.S. women aged 15–49 who use contraception—a smaller share than oral methods but clinically significant at population scale.
According to WHO classification data, meningiomas are typically graded WHO Grade I tumors, yet surgical resection rates climb when tumors enlarge or compress critical structures.
A 2024 *BMJ* study of French national health data reported that prolonged use of medroxyprogesterone acetate injectable contraception was associated with a 5.6-fold higher risk of intracranial meningioma requiring surgery among long-term users compared with non-users.
If you used Depo-Provera and were diagnosed with a brain tumor, you may have legal options.
Free, confidential Depo-Provera case review. Find out if you qualify.
Get a free Depo-Provera case reviewMeningiomas typically appear as well-defined, extra-axial masses on MRI scans, meaning they are located outside the brain tissue itself but within the skull. They often show characteristic features that help radiologists identify them, including their location, shape, and how they enhance with contrast agents. The MRI findings can provide important information about the tumor's size, location, and relationship to surrounding structures.
The imaging characteristics of meningiomas can vary, but they often show uniform enhancement after contrast administration, which helps distinguish them from other types of brain tumors. The location of the tumor on the meninges and its relationship to the brain tissue are key factors in both diagnosis and treatment planning.
Common MRI Findings in Meningioma Cases
MRI findings in meningioma cases typically show several characteristic features that help radiologists identify these tumors. Understanding these findings can help women who have been diagnosed with meningiomas after using Depo-Provera understand their imaging results.
A 2024 *BMJ* study of French national health data reported that prolonged use of medroxyprogesterone acetate injectable contraception was associated with a 5.6-fold higher risk of intracranial meningioma requiring surgery among long-term users compared with non-users.
According to WHO classification data, meningiomas are typically graded WHO Grade I tumors, yet surgical resection rates climb when tumors enlarge or compress critical structures.
According to FDA approval history, Depo-Provera (medroxyprogesterone acetate injectable suspension) has been marketed in the United States since 1992, with labeling updated multiple times as progestin safety data evolved.
Location: Meningiomas are typically found along the meninges, the protective layers surrounding the brain. They can occur in various locations, including along the convexity of the brain, at the base of the skull, near the falx cerebri, or along the tentorium. The location can affect both symptoms and treatment options.
According to FDA approval history, Depo-Provera (medroxyprogesterone acetate injectable suspension) has been marketed in the United States since 1992, with labeling updated multiple times as progestin safety data evolved.
Women who developed meningiomas after Depo-Provera injections may qualify for compensation.
No-cost evaluation for women who used Depo-Provera and developed a brain tumor.
Check your Depo-Provera eligibilityAppearance: On MRI scans, meningiomas typically appear as well-defined, rounded or lobulated masses. They often show uniform enhancement after contrast administration, which helps distinguish them from other types of brain tumors. The tumors may also show a characteristic "dural tail" sign, where the dura mater appears thickened adjacent to the tumor.
According to FDA approval history, Depo-Provera (medroxyprogesterone acetate injectable suspension) has been marketed in the United States since 1992, with labeling updated multiple times as progestin safety data evolved.
A 2024 *BMJ* study of French national health data reported that prolonged use of medroxyprogesterone acetate injectable contraception was associated with a 5.6-fold higher risk of intracranial meningioma requiring surgery among long-term users compared with non-users.
The National Brain Tumor Society notes that meningiomas account for roughly one-third of all primary brain tumors in adults—context that helps readers understand why even a modest relative risk increase can affect many patients.
Size and Growth: MRI scans can show the size of the meningioma and help track its growth over time. Some meningiomas may be small and stable, while others may grow larger and require treatment. Serial MRI scans can help monitor tumor growth and determine when intervention may be necessary.
The National Brain Tumor Society notes that meningiomas account for roughly one-third of all primary brain tumors in adults—context that helps readers understand why even a modest relative risk increase can affect many patients.
A 2024 *BMJ* study of French national health data reported that prolonged use of medroxyprogesterone acetate injectable contraception was associated with a 5.6-fold higher risk of intracranial meningioma requiring surgery among long-term users compared with non-users.
The National Brain Tumor Society notes that meningiomas account for roughly one-third of all primary brain tumors in adults—context that helps readers understand why even a modest relative risk increase can affect many patients.
According to WHO classification data, meningiomas are typically graded WHO Grade I tumors, yet surgical resection rates climb when tumors enlarge or compress critical structures.
A confidential case review can help you understand your Depo-Provera legal options.
No obligation. Understand your Depo-Provera legal options at no cost.
Request a free Depo-Provera evaluationEffects on Surrounding Structures: MRI findings can show how the meningioma affects surrounding brain structures. Larger tumors may cause compression of brain tissue, displacement of structures, or edema in surrounding areas. These findings help determine the urgency of treatment and the best approach.
According to FDA approval history, Depo-Provera (medroxyprogesterone acetate injectable suspension) has been marketed in the United States since 1992, with labeling updated multiple times as progestin safety data evolved.
If you've been diagnosed with a meningioma after using Depo-Provera, you may want to learn more about Depo-Provera lawsuit information and your potential rights.
Legal documents and research papers representing ongoing litigation
The Connection Between Depo-Provera and Meningiomas
Recent scientific research has revealed a connection between long-term Depo-Provera use and the development of meningiomas. A landmark French study published in the BMJ found that women who used high-dose progestogen medications like Depo-Provera for extended periods faced significantly elevated risks of developing these tumors.
According to CDC National Health Statistics Reports, injectable contraceptives are used by roughly 2% to 3% of U.S. women aged 15–49 who use contraception—a smaller share than oral methods but clinically significant at population scale.
According to WHO classification data, meningiomas are typically graded WHO Grade I tumors, yet surgical resection rates climb when tumors enlarge or compress critical structures.
According to FDA approval history, Depo-Provera (medroxyprogesterone acetate injectable suspension) has been marketed in the United States since 1992, with labeling updated multiple times as progestin safety data evolved.
Don't wait on your Depo-Provera claim—statutes of limitations may apply.
Get a free Depo-Provera case review and learn whether you may qualify.
See if you qualify for a Depo-Provera lawsuitThe study found that women who used Depo-Provera for extended periods, particularly five or more years, faced substantially higher risks of developing meningiomas compared to women who did not use the medication. The risk increased with the duration of use, indicating that cumulative exposure over time plays a significant role in tumor development.
The National Brain Tumor Society notes that meningiomas account for roughly one-third of all primary brain tumors in adults—context that helps readers understand why even a modest relative risk increase can affect many patients.
A 2024 *BMJ* study of French national health data reported that prolonged use of medroxyprogesterone acetate injectable contraception was associated with a 5.6-fold higher risk of intracranial meningioma requiring surgery among long-term users compared with non-users.
The research suggests that the hormone medroxyprogesterone acetate, the active ingredient in Depo-Provera, may play a role in the development of these tumors. While the exact mechanism is still being studied, the evidence indicates a clear association between long-term Depo-Provera use and increased meningioma risk. MRI findings in these cases can help establish the connection between medication use and tumor development.
What Is Depo-Provera?
Depo-Provera is an injectable contraceptive medication that contains the hormone medroxyprogesterone acetate. The medication is administered as an injection every three months to prevent pregnancy. It has been used by millions of women worldwide since its approval by the FDA in 1992.
According to FDA approval history, Depo-Provera (medroxyprogesterone acetate injectable suspension) has been marketed in the United States since 1992, with labeling updated multiple times as progestin safety data evolved.
The National Brain Tumor Society notes that meningiomas account for roughly one-third of all primary brain tumors in adults—context that helps readers understand why even a modest relative risk increase can affect many patients.
According to WHO classification data, meningiomas are typically graded WHO Grade I tumors, yet surgical resection rates climb when tumors enlarge or compress critical structures.
If you used Depo-Provera and were diagnosed with a brain tumor, you may have legal options.
Free, confidential Depo-Provera case review. Find out if you qualify.
Get a free Depo-Provera case reviewThe medication works by preventing ovulation and thickening cervical mucus to block sperm. While effective for birth control, emerging research has raised concerns about potential long-term health risks, particularly related to brain tumor development. Many women have used Depo-Provera for extended periods, sometimes for years or even decades, which may have contributed to the increased risk observed in recent studies.
According to FDA approval history, Depo-Provera (medroxyprogesterone acetate injectable suspension) has been marketed in the United States since 1992, with labeling updated multiple times as progestin safety data evolved.
Depo-Provera injections are typically administered by healthcare providers into the muscle of the arm or buttock. Each injection releases the hormone slowly over time, maintaining contraceptive effectiveness for approximately 12 to 14 weeks. The cumulative exposure from repeated injections over many years may be a factor in the increased meningioma risk observed in long-term users.
How Exposure Occurred
Women were exposed to Depo-Provera through regular injections administered by healthcare providers. The medication is typically injected into the muscle of the arm or buttock every 12 to 14 weeks. Each injection releases the hormone slowly over time, maintaining contraceptive effectiveness.
The National Brain Tumor Society notes that meningiomas account for roughly one-third of all primary brain tumors in adults—context that helps readers understand why even a modest relative risk increase can affect many patients.
A 2024 *BMJ* study of French national health data reported that prolonged use of medroxyprogesterone acetate injectable contraception was associated with a 5.6-fold higher risk of intracranial meningioma requiring surgery among long-term users compared with non-users.
The National Brain Tumor Society notes that meningiomas account for roughly one-third of all primary brain tumors in adults—context that helps readers understand why even a modest relative risk increase can affect many patients.
According to WHO classification data, meningiomas are typically graded WHO Grade I tumors, yet surgical resection rates climb when tumors enlarge or compress critical structures.
Women who developed meningiomas after Depo-Provera injections may qualify for compensation.
No-cost evaluation for women who used Depo-Provera and developed a brain tumor.
Check your Depo-Provera eligibilityExposure occurred through regular injections every three months, long-term use over multiple years, cumulative exposure building up over time, and direct injection into muscle tissue. Many women used Depo-Provera for extended periods, sometimes for years or even decades. This long-term, repeated exposure may have contributed to the increased risk of developing meningiomas observed in recent studies.
The National Brain Tumor Society notes that meningiomas account for roughly one-third of all primary brain tumors in adults—context that helps readers understand why even a modest relative risk increase can affect many patients.
The cumulative nature of the exposure is particularly important when considering the development of meningiomas. The hormone builds up in the body over time with each injection, and women who received injections for many years may have had significantly higher cumulative exposure than those who used the medication for shorter periods. MRI findings can help document the presence of these tumors and their characteristics.
Evidence and documents in legal proceedings
Who May Be Affected
Women who used Depo-Provera for extended periods may be at increased risk of developing meningiomas. Research suggests that the risk increases with the duration of use. Women who used the medication for one to four years may face a moderate increase in risk, while those who used it for five or more years may face significantly higher risks. Women who used it for ten or more years may face the highest risks.
According to WHO classification data, meningiomas are typically graded WHO Grade I tumors, yet surgical resection rates climb when tumors enlarge or compress critical structures.
According to FDA approval history, Depo-Provera (medroxyprogesterone acetate injectable suspension) has been marketed in the United States since 1992, with labeling updated multiple times as progestin safety data evolved.
A 2024 *BMJ* study of French national health data reported that prolonged use of medroxyprogesterone acetate injectable contraception was associated with a 5.6-fold higher risk of intracranial meningioma requiring surgery among long-term users compared with non-users.
A confidential case review can help you understand your Depo-Provera legal options.
No obligation. Understand your Depo-Provera legal options at no cost.
Request a free Depo-Provera evaluationThe French study found that women who used high-dose progestogen medications for more than a year had a significantly elevated risk, with some groups facing risks more than five times higher than non-users. Women who have been diagnosed with meningiomas after using Depo-Provera, as confirmed by MRI findings, should consider having their situation evaluated to determine whether they may have a valid legal claim.
A 2024 *BMJ* study of French national health data reported that prolonged use of medroxyprogesterone acetate injectable contraception was associated with a 5.6-fold higher risk of intracranial meningioma requiring surgery among long-term users compared with non-users.
If you've used Depo-Provera for an extended period and have been diagnosed with a meningioma based on MRI findings, you may want to learn more about Depo-Provera lawsuit information and your potential rights.
Current Status of Litigation
Litigation related to Depo-Provera and meningiomas is developing as more women learn about the potential connection between their medication use and brain tumor diagnosis. Cases are being filed alleging that manufacturers knew about the risks but failed to adequately warn patients and healthcare providers.
The National Brain Tumor Society notes that meningiomas account for roughly one-third of all primary brain tumors in adults—context that helps readers understand why even a modest relative risk increase can affect many patients.
According to FDA approval history, Depo-Provera (medroxyprogesterone acetate injectable suspension) has been marketed in the United States since 1992, with labeling updated multiple times as progestin safety data evolved.
The litigation is in early stages, with cases being filed in various courts. As more scientific evidence emerges and more women come forward, the litigation may develop into consolidated proceedings similar to other pharmaceutical mass tort cases. Scientific evidence continues to accumulate linking progestogen exposure to meningioma development, and MRI findings play an important role in documenting these cases.
According to FDA approval history, Depo-Provera (medroxyprogesterone acetate injectable suspension) has been marketed in the United States since 1992, with labeling updated multiple times as progestin safety data evolved.
Don't wait on your Depo-Provera claim—statutes of limitations may apply.
Get a free Depo-Provera case review and learn whether you may qualify.
See if you qualify for a Depo-Provera lawsuitEvidence suggests that the risks associated with progestogen exposure were known for years before adequate warnings were provided. Pharmaceutical companies have a legal obligation to warn patients and healthcare providers about known risks. If you've used Depo-Provera for an extended period and developed a meningioma, as documented by MRI findings, you may be entitled to compensation for medical expenses, lost wages, pain and suffering, future medical care, and reduced quality of life.
What a Case Review Involves
A case review is an initial evaluation to determine whether you may have a valid legal claim related to Depo-Provera use and meningioma development. This process is confidential, free, and does not create any obligation on your part.
According to WHO classification data, meningiomas are typically graded WHO Grade I tumors, yet surgical resection rates climb when tumors enlarge or compress critical structures.
The National Brain Tumor Society notes that meningiomas account for roughly one-third of all primary brain tumors in adults—context that helps readers understand why even a modest relative risk increase can affect many patients.
According to FDA approval history, Depo-Provera (medroxyprogesterone acetate injectable suspension) has been marketed in the United States since 1992, with labeling updated multiple times as progestin safety data evolved.
Initial Consultation: The process typically begins with a conversation about your Depo-Provera use history and medical diagnosis. You'll be asked about when you started using Depo-Provera, how long you used it, when you received your meningioma diagnosis, and what symptoms you've experienced. MRI findings and imaging reports may be important documentation in evaluating your potential claim.
Medical Records Review: If you decide to proceed, medical records related to your meningioma diagnosis and treatment may be reviewed. This includes MRI reports and imaging studies that document the presence and characteristics of the tumor. This helps establish the connection between your medication use and your condition. You may also be asked about your Depo-Provera injection history and any documentation you have.
According to WHO classification data, meningiomas are typically graded WHO Grade I tumors, yet surgical resection rates climb when tumors enlarge or compress critical structures.
If you used Depo-Provera and were diagnosed with a brain tumor, you may have legal options.
Free, confidential Depo-Provera case review. Find out if you qualify.
Get a free Depo-Provera case reviewA 2024 *BMJ* study of French national health data reported that prolonged use of medroxyprogesterone acetate injectable contraception was associated with a 5.6-fold higher risk of intracranial meningioma requiring surgery among long-term users compared with non-users.
According to WHO classification data, meningiomas are typically graded WHO Grade I tumors, yet surgical resection rates climb when tumors enlarge or compress critical structures.
Eligibility Assessment: Based on the information gathered, including MRI findings, an assessment will be made about whether you may qualify to pursue a claim. Factors considered include the duration of your Depo-Provera use, the timing of your diagnosis, the characteristics of your meningioma as shown on MRI, and how your case fits within the broader litigation.
Next Steps: If you may qualify, you'll be informed about the next steps in the legal process. This might include connecting you with an independent law firm that handles Depo-Provera cases. If you don't qualify, you'll receive an explanation of why.
A 2024 *BMJ* study of French national health data reported that prolonged use of medroxyprogesterone acetate injectable contraception was associated with a 5.6-fold higher risk of intracranial meningioma requiring surgery among long-term users compared with non-users.
No Upfront Costs: Case reviews are conducted at no cost to you. If you qualify and choose to proceed with a case, most attorneys work on a contingency fee basis, meaning they only receive payment if your case is successful. To understand more about how mass tort cases work, you may find our guide on understanding mass tort litigation helpful.
According to FDA approval history, Depo-Provera (medroxyprogesterone acetate injectable suspension) has been marketed in the United States since 1992, with labeling updated multiple times as progestin safety data evolved.
A 2024 *BMJ* study of French national health data reported that prolonged use of medroxyprogesterone acetate injectable contraception was associated with a 5.6-fold higher risk of intracranial meningioma requiring surgery among long-term users compared with non-users.
The case review process is designed to be straightforward and respectful of your situation. The goal is to help you understand your options and determine whether pursuing legal action makes sense for your circumstances. If you're ready to begin, you can contact us for a free case review.
Women who developed meningiomas after Depo-Provera injections may qualify for compensation.
No-cost evaluation for women who used Depo-Provera and developed a brain tumor.
Check your Depo-Provera eligibilityImaging is evidence—not a verdict
Radiology reports establish size, location, and growth patterns, but lawyers still must connect those findings to product use and warnings. Keep DICOM discs and radiology notes for your review appointment.
The National Brain Tumor Society notes that meningiomas account for roughly one-third of all primary brain tumors in adults—context that helps readers understand why even a modest relative risk increase can affect many patients.
Scientific Evidence: While research suggests a link between Depo-Provera and meningiomas, scientific evidence continues to evolve. Courts will evaluate this evidence, and outcomes may depend on how juries and judges interpret the available research and MRI findings.
According to WHO classification data, meningiomas are typically graded WHO Grade I tumors, yet surgical resection rates climb when tumors enlarge or compress critical structures.
Litigation Timeline: Mass tort litigation typically takes several years to resolve. Cases may proceed through discovery, expert witness preparation, and potentially trials or settlement negotiations. The timeline for your specific case depends on many factors beyond your control.
See if you qualify for a free case review to learn more about your potential rights and options. You can also learn more about Depo-Provera lawsuit information and your potential rights.
Important Disclaimers
MRI findings play an important role in diagnosing meningiomas in women who have used Depo-Provera. If you've used Depo-Provera for an extended period and have been diagnosed with a meningioma based on MRI findings, understanding your legal rights and options is an important first step.
A confidential case review can help you understand your Depo-Provera legal options.
No obligation. Understand your Depo-Provera legal options at no cost.
Request a free Depo-Provera evaluationAccording to WHO classification data, meningiomas are typically graded WHO Grade I tumors, yet surgical resection rates climb when tumors enlarge or compress critical structures.
The National Brain Tumor Society notes that meningiomas account for roughly one-third of all primary brain tumors in adults—context that helps readers understand why even a modest relative risk increase can affect many patients.
A 2024 *BMJ* study of French national health data reported that prolonged use of medroxyprogesterone acetate injectable contraception was associated with a 5.6-fold higher risk of intracranial meningioma requiring surgery among long-term users compared with non-users.
Mass tort and product cases often involve complex science and procedure. This page explains one piece of the puzzle; a case review addresses how it may apply to you.
Top Tier Legal, LLC is not a law firm and does not provide legal advice. This content is for informational purposes only. Submitting information does not create an attorney-client relationship. If you qualify, Top Tier Legal, LLC may connect you with an independent law firm. Past results do not guarantee future outcomes.


